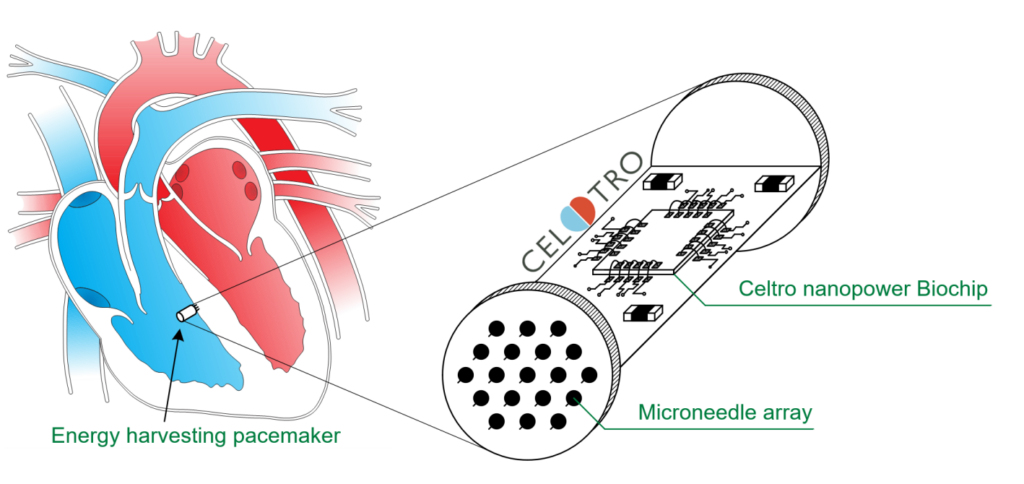
Functional Silicon for autonomous Pacemaker
May, 2026 – Celtro is developing solutions for energy harvesting from human tissue to supply medical implants in the human body. To this purpose, a

Gerd Teepe, PhD

Jarek Budny, MBA

Paul Reidy, Esq

Forrest Pape, MSEE

Thomas Gaspar, MD

Judith Piorkowski, MD

Mike Pederson, MBA

Prof. Dr. Kai Simons